From the moment a baby is born, and even before birth during the 9 months his mother is carrying him, a baby is designed to develop attachment with a nurturing caregiver. When a baby’s needs are provided for and mom or dad looks loving into his eyes, talks to him, and shows loving care, a baby learns to trust.
When this amazing process does not happen due to neglect, a mother’s depression, or early childhood trauma or abuse, a child is at risk for developing attachment issues or Reactive Attachment Disorder (RAD). What is RAD, and why should you care?
What is Reactive Attachment Disorder (RAD)?
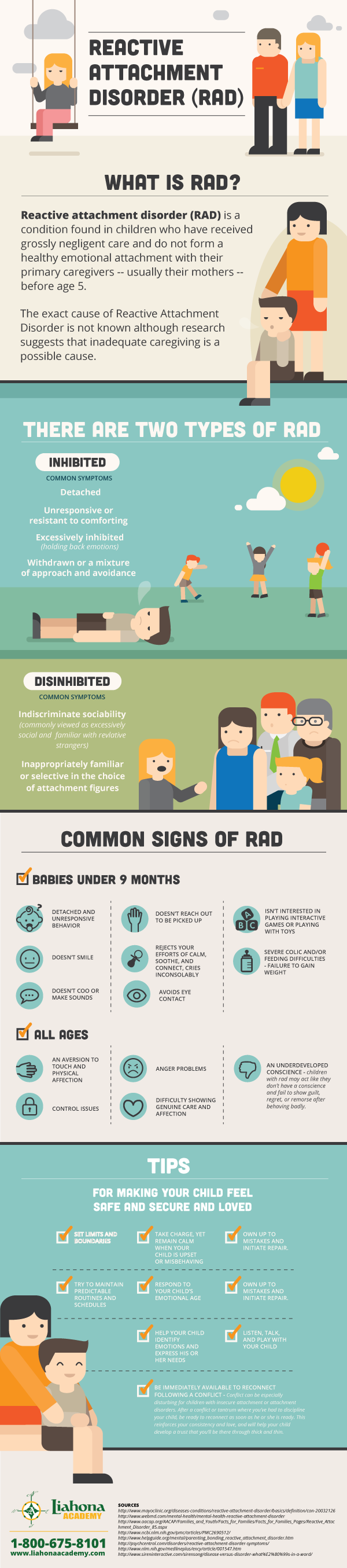
Reactive Attachment Disorder (RAD) is defined as a problematic pattern of developmentally inappropriate moods, social behaviors, and relationships due to a failure to form normal, healthy attachments with primary caregivers in early childhood.
A child who experiences neglect, abuse, or separation during the critical stages of development during first three years of life is at risk of developing an attachment disorder.
Remember, only a qualified doctor or trained therapist can diagnose an attachment disorder.
Are you gift shopping for a child who has attachment issues? Be sure to check out our post, 15 Gifts that Promote Attachment and Bonding to find an idea present, while also promoting healthy relationships.
Causes of Reactive Attachment Disorder (RAD)
While study is ongoing, the following are reasons why a child might have an attachment disorder:
- Early childhood trauma or abuse
- No primary caregiver or a depressed primary caregiver
- Medical procedures during the first years of life
- Neglect during the first years of life
RAD is typically seen in children who have been abused, neglected, or experienced trauma from newborn to 3 years of age. Reactive Attachment Disorder is often seen in children who have been in foster care or adopted from other countries, but that is not always the case. RAD is also seen in biological children or within step-families.
Types of Attachment Disorder
There are now two sub-types of attachment disorders – emotionally withdrawn/inhibited and indiscriminately disinhibited, defined separately in the DSM-V as distinct disorders:
- Reactive Attachment Disorder (RAD)
- Disinhibited Social Engagement Disorder (DSED).
Reaction Attachment Disorder is diagnosed when a child’s relationships are inhibited and the child fails to engage in social interactions in an appropriate developmental way.
Disinhibited Social Engagement Disorder (DSED) is diagnosed when a child does not have an appropriate attachment to primary caregivers but instead will attempt to form relationships with strangers.
Signs of Attachment Disorder in Infants
- Avoids eye contact
- Doesn’t smile
- Doesn’t reach out to be picked up
- Rejects your efforts to calm, soothe, and connect
- Doesn’t seem to notice or care when you leave them alone
- Cries inconsolably
- Doesn’t coo or make sounds
- Doesn’t follow you with his or her eyes
- Isn’t interested in playing interactive games or playing with toys
- Spend a lot of time rocking or comforting themselves
Symptoms of Reaction Attachment Disorder (RAD)
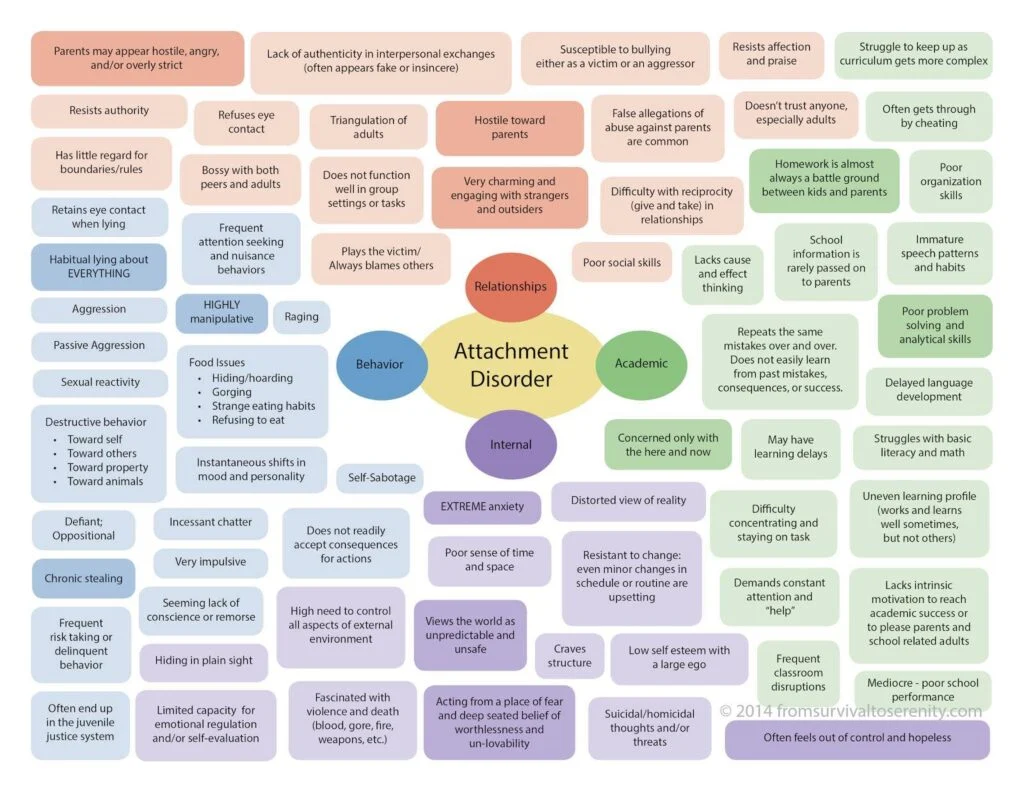
RAD is diagnosed when a child’s social relations are inhibited and, as a result, he/she fails to engage in social interactions in a manner appropriate to his/her developmental age.
The child may show:
- avoidance
- hyper-vigilance or
- resistance to social contact
- avoid social reciprocity
- fail to seek comfort when upset
- become overly attached to one adult
- refuse to acknowledge a caregiver
Symptoms of Disinhibited Social Engagement Disorder (DSED)
DSED is diagnosed when a child is:
- excessively social with strangers
- does not engage in selective attachments
- indiscriminately engage in social behavior
RAD (Reactive Attachment Disorder) was originally the only diagnostic measure for children with unhealthy attachment. In recent years, as more about attachment has come to light, the subsets of RAD and DSED have been added.
I believe that in the future, different and more specific terms will be used, but as of today, these remain the standard criteria for this complex disorder.
In the next post in this series, I’ll share more information about types of unhealthy attachment issues, what it mean in day-to-day life, and getting treatment.
Why Should You Care About Reactive Attachment Disorder (RAD) and How Can You Help?
The diagnostic descriptions of Reactive Attachment Disorder to do not begin to explain what everyday life is like for the families and children who live with these realities. Families who are raising children with RAD, DSED, or attachment issues need your support.
As with many mental health disorders, these diagnoses are often not isolated. Many children with RAD also deal with PTSD, Oppositional Defiant Disorder, ADHD, depression, and other mental health challenges.
Understanding is critical. Many of the parenting strategies that generally work for typical child are not effective for a child who has Reactive Attachment Disorder.
Parents and siblings often deal with Secondary PTSD.
At the extreme end of the attachment disorder continuum, children have the capacity to develop without consciousness, which leads to psychopathic tendencies if treatment is not effective. Parents who are raising children with RAD, caregivers, teachers, and therapists deserve our support and funding. They are working to heal the hearts of these children so they can be safe, productive members of society.
As one of my friends says about her son, who is healing from RAD, “We are teaching him how to love.”
Are you parenting a child with RAD (Reactive Attachment Disorder)? Please share your insights in the comments below. What do you wish people knew?
More Helpful Posts to Navigate Reactive Attachment Disorder (RAD):
RAD Checklist: What Does Reactive Attachment Disorder Look Like?
Can a Child Heal from RAD? Answers to Questions about Reactive Attachment Disorder
Reactive Attachment Disorder (RAD) Treatment Centers – Listing by State




Leave a Reply